
Annual Meeting held March 10th
March 31, 2015
A gala annual meeting of Healthcare-Now of Maryland was held March 10th, 2015 at the Episcopal Diocese of Maryland in Baltimore. Forty-five members and friends of single-payer were in attendance. Speakers summarized activities of the past year–participation in Lobby Day in Annapolis, marching in the annual MLK Day parade in Baltimore, and grants to the Healthcare is a Human Right Campaign Maryland. Eric Naumburg gave an update on the latter campaign. Robert Zarr, president of PNHP, gave the featured address, which highlighted personal experiences with community health that encouraged physician endorsement of single-payer. Bumper stickers, buttons, and literature were on sale. Plans for the rest of 2015 were unveiled. All are invited to attend monthly meetings also held at the Episcopal Diocesan Center, usually on the fourth Thursday of the month.
Want to show “The Healthcare Movie”?
April 27, 2014
Want to show “The Healthcare Movie” at a house party to your friends, family, neighbors, club, or church, etc.? The movie has dynamic comparisons of Canada vs. USA healthcare. Healthcare-Now of Md. will get you (that is, mail or, if in the Baltimore area, deliver to you a free copy for the showing. Either the 65 minute or 25 minute version. Also, we’ll be happy to have one of our members lead a discussion and answer questions.
For more info, or to make arrangements, email info@mdsinglepayer.org.
Health Justice March Gets Media Coverage
November 24, 2013
On a beautiful, crisp fall day folks from all around Maryland came to Baltimore and marched from Patterson Park to Canton, across from the First Mariner building where Carefirst, the largest private insurer in Maryland and symbol of what’s wrong with healthcare has offices. The march called attention to the serious problems Marylander’s have in getting and paying for healthcare; there are over 750,000 without insurance and medical illness remains the number one cause of personal bankruptcy. Many delay seeking care because of cost. We are asking Maryland to treat healthcare as a human right and make it a public good like our roads, the police and firefighters and not commoditify it as a source of profit for investors and CEO’s.
Lead by a marching band, the “Christian Warriors”, the march brought many people out of their houses. Flyers explaining the purpose of the march were passed out and many told us they supported a publicly financed universal healthcare system, everybody in and nobody out. The event included street theater where the dragon of death, signifying the fate of the uninsured was routed by the strength of people coming together and demanding their rights.
The march was covered by the Baltimore Sun, Channel 11, The Real News and several local newspapers.
At the event, we announced the formation of a statewide leadership council which will help direct our campaign.
Link to coverage of the Health Justice March: http://healthcareisahumanrightmaryland.org/campaign/blog/media-healthcare-march
Maryland Economic Impact Study by Gerald Friedman, Ph.D.
July 22, 2012
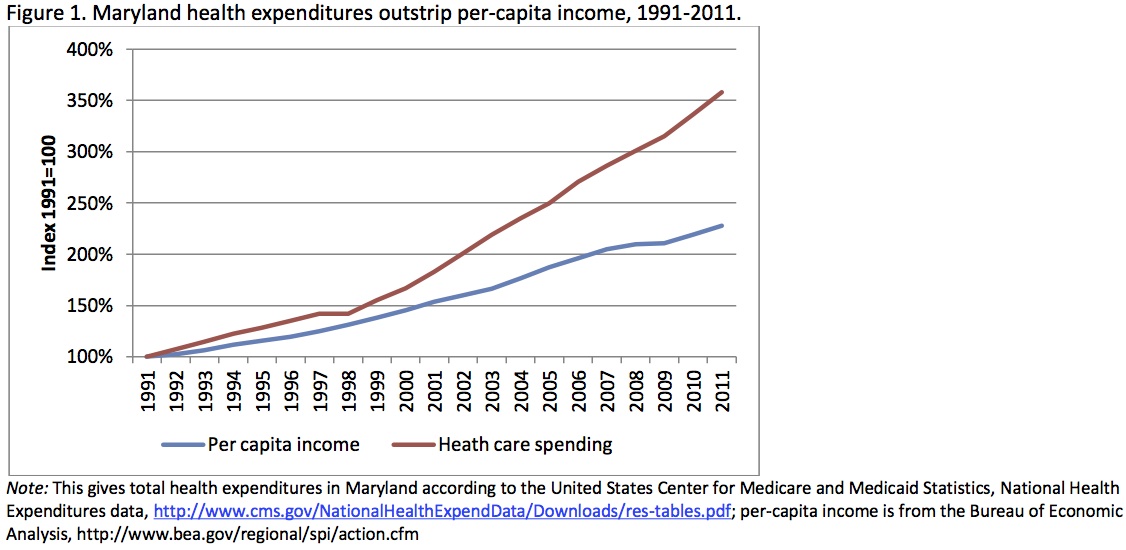
The following is the executive summary of the economic impact study of the proposed Maryland Health Security Act. You can download the full study here.
Maryland is on an unsustainable economic path; health care costs are absorbing a growing share of personal income. Between 1991 and 2011, health care spending in Maryland increased by $35 billion, nearly 10-times the rate of population growth and almost twice the rate of growth in per-capita income. Should health care spending continue to increase at this rate, spending will pass $100 billion in a little over a decade. Little of this increased spending can be attributed to improvements in health care; instead, the fastest growth has been in administration and billing operations while many remain without adequate health insurance or access to needed care.
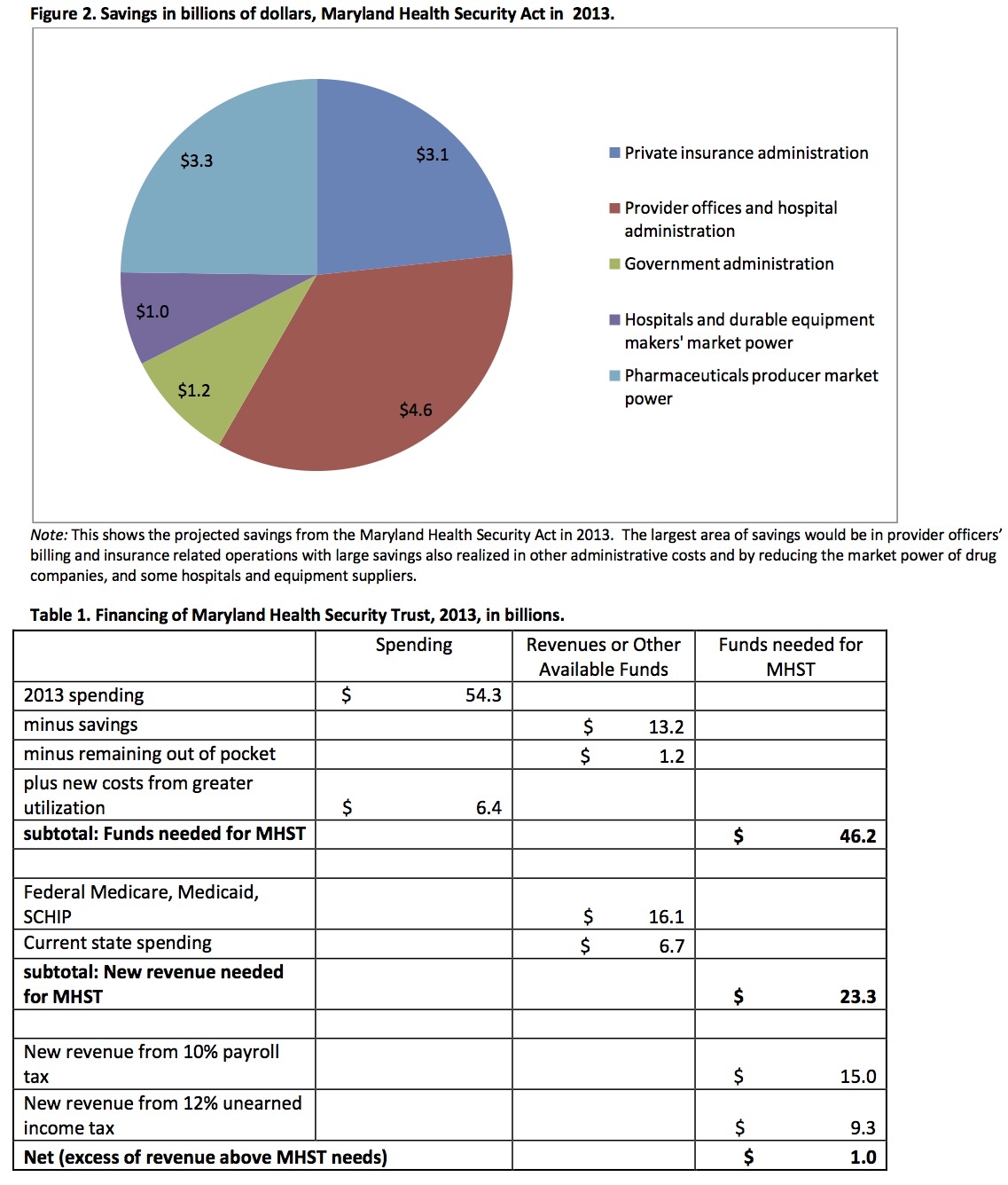
The Maryland Health Security Act (MHSA) would put Maryland on a sustainable path by controlling health care costs while giving all citizens access to quality health care. It would establish the Maryland Health System Trust (MHST) as a single-payer system to finance health care, paying for all necessary medical care including hospital care, visits to doctors, nurses, occupational and physical therapy, prescription drugs, medical devices, medically necessary nursing home care and home health care. By reducing administrative costs and anti- competitive market practices, the MHST could save over $13.2 billion in 2013, or over 24% of existing spending. These savings would allow the expansion of coverage to all Maryland residents while still saving over $6 billion, or over $1,000 per person.
The MHST would be funded by payroll taxes and a levy on non-wage income including capital gains, profits, rents, dividends, and interest. The shift from insurance premiums and out-of-pocket expenses to taxes linked with income would especially benefit lower- and middle-income Marylanders, businesses would also benefit from the reduced administrative burden and because payroll taxes would be less than most now pay in insurance. By lowering payroll costs, the MHST would make Maryland businesses more competitive, producing an additional 70,000 new jobs.
Pharmed Out: U.S. Practitioners and Big Pharm Harm More Than They Heal
June 18, 2012
U.S. Practitioners and Big Pharm Harm More Than They Heal, Notes from conference June 14-15, 2012.
An Article by Dr. Deborah Schumann, M.D. from conference at Georgetown, University.
Marketing: Americans spend 100 times more time exposed to drug and device ads than they spend face to face with their doctors. Barbara Mintzes, PhD. Therapeutic Initiative, Vancouver, Canada.
Drug mortality: Appropriately prescribed pharmaceuticals are the 4th leading cause of death in the U.S., while 2% of drugs are “life-saving.” Donald Light, PhD., University of Medicine and Dentistry of New Jersey.
For full article click on Pharmed Out:.
New Chapter Meetings Begun in Montgomery County
January 17, 2012
Montgomery County Healthcare-NOW, led by several PNHP members, met April 10 at Dr. Deborah Schumann’s home. Our volunteer membership brings together a broad range of experience in primary and specialty care, health care policy, employee benefits management, and community health care organizing and delivery. Our immediate plans include organizing for local participation in the Health Care is a Human Right campaign. For this, we need both medical and non-medical people who want to help us achieve equal access to affordable quality health care for all.
Check us out. For contact info go to http://www.mdsinglepayer.org/about/contact-us/
Groups meeting in Carroll, Frederick and Calvert County
January 12, 2012
The Maryland Healthcare is a Human Right! now has groups meeting in 7 localities and counting. Recently, groups in Carroll, Frederick and Calvert County have formed, in addition to Baltimore City, Howard, Montgomery and Anne Arundel County. The campaign is opening a new website http://healthcareisahumanrightmaryland.org (apologies for long URL), in order to centralize information and create new branding for the campaign. The campaign colors are red, yellow, black and white, i.e. Maryland’s state colors.
Currently, the emphasis of many advocates is on building up and expanding the campaign. We need a much larger base of support; so that when we start emphasizing the legislature they will notice and listen. With energy and time having its limits, there will be a decreased emphasis on legislation this session. There is no plan to re-introduce the Maryland Health Security Act this year. This will disappoint some. However, for those wanting to keep the single-payer fires burning in Annapolis, there will be the opportunities to testify on the exchange legislation. We know single-payer is superior in every way to the current and newly forming health insurance system. Meanwhile don’t hesitate to communicate with your state senators and delegates about single-payer and the Friedman study “Financing the Maryland Health Security Act”, available on this website. There is also a link to the Maryland Health Security Act from 2011 which is identical to the 2012 version if want to refer to it.
–Eric Naumburg, M.D., M.P.H. 12/12/12
Single-payer system would alleviate misuse of emergency rooms
June 4, 2011
Baltimoresun.com
4:37 PM EDT, June 1, 2011
The headline reads emergency room visits at Howard County General Hospital “might hit a high mark” this year. We know this means that the ER is being misused as a source of primary care. Don’t feel bad, Howard County; in Massachusetts, the model for national health reform, emergency room visits hit a new high last year, and they have under 5 percent with no health insurance, while Maryland has a close to 15 percent uninsured.
The overuse of the ER is a symptom of the lack of primary-care providers in the county. Why the shortage? It is our faith in the markets to make things work. Health Insurers have the upper hand; they decide what primary care is worth. The result is the pay is too low to attract enough primary-care providers.
The reliance on a profit-driven market place to make the medical system work is a problem beyond a shortage of primary care in wealthy county like Howard. The cost of health insurance has more than doubled in the past nine years and the employee share of this expense is rising. Wages have not and cannot keep up with this pace. Before too long most of our salaries will be going to health insurance.
There is a better solution. It is a single-payer health-care system, a program like Medicare that includes everyone but with expanded coverage. The administrative waste in health care is staggering. We spend over 1/3 of our health care dollars on it. Administrative hassles eat up over 10 percent of our doctors’ time that could be put to patient care. A government-run, taxpayer-financed privately delivered system would eliminate much of this waste.
The payment system is streamlined; the middle man (health insurers) is gone. Decisions about doctor pay and distribution of resources can now be made based on medical need first and then profit. With the savings, health-care coverage could be made universal, and expanded to include all needed medical services plus dental and pharmacy. The academic studies to prove this have been done, repeatedly. More importantly, international experience with single-payer systems show the same outcome.
Vermont has passed legislation that will lead to universal health care based on a single-payer system in their state. The Vermont bill starts from the principle that access to health care is a human right. Right now, health care is being treated as a commodity, rationed based on ability to pay. Maryland has similar legislation to Vermont; the Maryland Health Security Act (SB 388). I urge you to find out about it.
Eric Naumburg
Columbia
Eric Naumburg, M.D., is Maryland Health Security Act coordinator for Healthcare-Now of Maryland.
www.baltimoresun.com/explore/howard/opinion-talk/letter-editor/ph-ho-cf-letters-060211-7-20110601,0,818858.story
Contact your State Legislators about the MD Health Security Act Now
May 30, 2011
Healthcare-Now of Maryland makes it easy for you to ask your state legislators to support the Maryland Health Security Act.
Teams of Healthcare-Now of Maryland members have been in Annapolis the past few weeks meeting with state legislators and asking for their support. Of course, as a constituent, your voice is more powerful than ours. That is why we need your help.
Please visit the new page on our website and take a moment to send a note to your state delegate(s) and senator. It only takes a few minutes. You can use our letter or write your own. You don’t even need to know who your state legislators are. Healthcare-Now will find out for you, based on your address, and will provide you with their names and photos. Just go here.
Thank you for taking the time to support the Maryland Health Security Act.
Contact Your Member of Congress About Funding Domestic Needs
May 16, 2011
Healthcare-Now of MD is a member of the Fund Our Communities campaign to cut military spending and fund domestic priorities such as universal health care, education and jobs. Forty members of the Maryland state legislature signed on to a letter that was sent to all Maryland members of Congress asking them to decrease military spending and instead use the tax dollars to repair our crumbling social and physical infrastructure. You can read the letter here (.pdf).
We are asking you to take a moment to contact your Maryland senators and representative to offer support for this letter. You can do so by clicking here.
Sign Up
Sign up for our free email list to receive updates.

Volunteer
To get the Healthcare is Human Right Campaign rolling we are going to need lots of volunteers. Please go to our Take Action Page and tell us how can help. There are many different kinds of opportunities. Thanks.

Donate
Time to Join or Renew Membership in Healthcare-Now of Maryland.
Donate here online $20 which covers 2021 dues. Or mail check with your snail address for $15.00. Either way, just click "Donate" and follow instructions.

Join our Facebook group.
![]()
In the News
-
MLK Day parade, January 16, 2017
 Healthcare-NOW!
Healthcare-NOW!- PNHP
